
Toxoplasmosis
Toxoplasmosis is an infection that between 30 and 80% of the healthy population undergoes during their lifetime.
In Europe, it usually proceeds without clinical symptoms, i.e. when the immune system is healthy. Occasionally, however, it is experienced as a febrile illness with fatigue and swelling of the lymph nodes over several weeks. In other continents, especially in South America, much more aggressive courses are the rule, here every second person suffers from eye involvement.
-
GENERAL, EXPLANATION OF TERMS
Toxoplasma gondii, the causative agent of toxoplasmosis, is a parasite of the earth’s surface that can be found on practically all continents. In its very environmentally resistant cyst form it resists both heat and desiccation, which has contributed to its widespread distribution. It is taken up by the earth’s surface with food, including herbivores (vegetarians), and quickly changes into its active form; the tachyzoites, in the body of its host. It penetrates the bloodstream and almost all tissues of the body. There it can multiply until the host’s immune system has gained control of the pathogen. Humans almost never notice the infection, whereas it can be fatal in some animal species, especially rodents. The infection induces the formation of antibodies. The pathogen is now attacked by the immune system and forced to hide in the tissue. To do this, it changes into a new form of survival, the tissue cysts, which can no longer be reached by the body’s own defense system. The cysts now rest for life in almost all host tissues and the parasite waits for a favorable opportunity, for example a weakness of the immune system, to become active again.
-
ACQUIRED TOXOPLASMOSIS
Rodents and birds pass on the pathogen in its tissue cysts to other carnivores and cats at some point in the food chain. Only in animals such as cats can the pathogen, (via a sexual reproductive step), pass back into the environmentally resistant cysts. They are then excreted in large quantities by the infected cats and hence distribution over the entire surface of the earth. Since the cat is not the only carrier of the infection, keeping away from them does not (as was long believed) mean protection from the infection. In our latitudes, most people ingest the pathogen with their food, especially with not completely cooked meat. Only in direct contact with cat excrement or soil, for example in a sandbox or while working in the garden, can the ingestion of a cyst lead to infection. Which is why it is not uncommon for vegetarians to get infected. The cysts dissolve in the stomach and intestines, and the pathogen penetrates the gastrointestinal wall and the bloodstream. This is how the acquired toxoplasmosis develops.
-
PREGNANCY
The infection, which is generally unproblematic, can actually become a problem in Europe if it is acquired for the first time during pregnancy. Then the pathogen can be transmitted to the unborn child via the bloodstream and placenta. With its immature immune system, the child is not yet able to protect itself sufficiently, so that the pathogen can spread to the brain and eyes and cause serious damage.
By the end of life, the majority of people are infected with toxoplasmosis. If antibodies are present in the mother’s blood at the beginning of pregnancy, this means the infection was already in the body before pregnancy and that the immune system usually controls the pathogen sufficiently. The child is thus protected against transmission of the infection. Between the ages of 20 and 40, two thirds or more of women in Northern and Central Europe are not yet infected, i.e. seronegative. This means they theoretically have a risk of up to 1% of acquiring toxoplasmosis during pregnancy. In about one third of these pregnancies the infection is transmitted to the child, which then develops congenital toxoplasmosis. Whether the child is clinically healthy or seriously ill or develops signs of disease during life depends on the age of the pregnancy at the time of infection of the child. Preventive diagnosis of the pregnant woman for early detection of the new infection, which is not noticed by the mother, is suitable for treating the infection early on, i.e. during pregnancy, with therapy for mother and child.
Only 10 to 25% of congenitally infected children in Europe show signs of infection at birth. At birth, however, eye involvement is found in as many as 8% and calcifications in the brain in 1%. Severe infections leading to infant death are very rare today. The congenital infection leads to the colonization of all tissues, especially the healthy retina with tissue cysts. An inflammatory flare in the eye area occurs at some point in the course of life, presumably as a result of the bursting of the tissue cysts and the release of the parasites.
-
SYMPTOMS
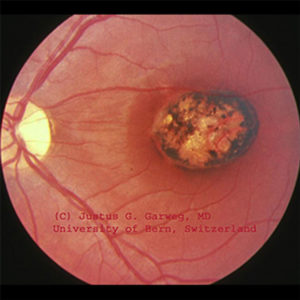 Typical macular scar on the left eye of a 12-year-old, otherwise healthy boy with a known congenital toxoplasmosis which "only" affected the eyes. Due to the scar at the site of sharpest vision (macula), the visual acuity of this eye is reduced to finger counting and spatial orientation, but the visual field is normal.
Typical macular scar on the left eye of a 12-year-old, otherwise healthy boy with a known congenital toxoplasmosis which "only" affected the eyes. Due to the scar at the site of sharpest vision (macula), the visual acuity of this eye is reduced to finger counting and spatial orientation, but the visual field is normal.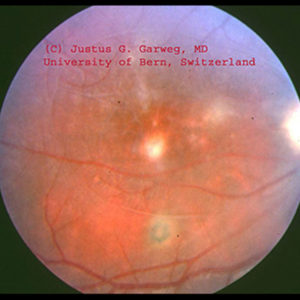 Same patient as above. Several scars can be seen on the retina of the right eye which show that the inflammation has been active several times (recurrences). The white, blurred focus directly next to the site of sharpest vision is a fresh recurrence, which the patient noticed while still having quite good visual acuity, mainly due to the clouding in front of the retina. These changes, often perceived like mosquitoes in front of the eye, are caused by the shadows of the inflammatory cells inside the eye.
Same patient as above. Several scars can be seen on the retina of the right eye which show that the inflammation has been active several times (recurrences). The white, blurred focus directly next to the site of sharpest vision is a fresh recurrence, which the patient noticed while still having quite good visual acuity, mainly due to the clouding in front of the retina. These changes, often perceived like mosquitoes in front of the eye, are caused by the shadows of the inflammatory cells inside the eye.Both congenital and acquired toxoplasmosis can cause symptoms and diseases of the eye. It is not yet known which factors favor an infestation of the eyes. The resulting inflammation of the interior of the eye (retinochoroiditis) or chorioretinitis = inflammation of the retina and choroid) poses a threat to the vision of the affected eye. This is because if the center of the retina (macula) is affected, the reading ability of the eye is threatened and can be lost. Direct involvement of the macula is found in up to 30% of both forms of toxoplasmosis, but probably less frequently in acquired ocular toxoplasmosis. When the macula is destroyed by toxoplasmosis, straight vision is usually very poor (larger objects can only be recognized by looking past them rather than directly at them), but the field of vision is largely normal. As a consequence, strabismus can occur.
A further problem with eye infestation is that the disease, which in otherwise healthy patients lies dormant as an inactive disease, can flare up in the eye without any predictable signs or causes. It can cause new visual disturbances and a further threat to vision.
Involvement of the second eye is not uncommon, especially if scars are already present. However, bilateral visual disturbances are very rare today, and obviously also influenced by whether or not treatment is given during the first year of the child’s life with confirmed toxoplasmosis. If the second eye has no source of virus in the middle of the retina, the risk is even lower. However, even if there is a source in the middle of the retina, the second eye can usually maintain very good visual acuity if diagnosed in time.
-
DIAGNOSTICS
The diagnosis of ocular toxoplasmosis from serum (blood) is not possible. If there is any doubt about the diagnosis, a parallel examination of blood and aqueous humor (fluid of the inner eye) can confirm the diagnosis in most cases.
-
TREATMENT
There are various antibiotics available for the treatment of ocular toxoplasmosis, but their major common problem is poor tolerability. For this reason, treatment is not recommended in every case, but is advisable if there is a threat to visual function. For the typical treatment of ocular toxoplasmosis, a combination of two antibiotics are most commonly prescribed. Daraprim ® and Sulfadiazine ® or a combination preparation such as Cotrim forte ® must be given for several weeks. However, this is not able to kill the pathogen, but only to convert the active form into a dormant form. One argument in favor of treatment is that patients who are treated probably experience fewer relapses than patients who are not treated. So far, there is no clinical, but at least animal experimental evidence for this. In addition to the above-mentioned therapy, folic acid (e.g. Lederfolat) is often prescribed to support blood formation, especially in pregnant women. This neutralizes the effect of antibiotic therapy and should be avoided at all costs. The addition of the considerably more expensive folinic acid, on the other hand, supports the effect of the antibiotics and is to be considered useful for the treatment of toxoplasmosis.
Only rarely does ocular toxoplasmosis lead to secondary problems of the eye such as cataracts or glaucoma and retinal detachment. Whereas disturbing vitreous opacities are always observed at the beginning, then usually disappear again to a large extent.
In congenital toxoplasmosis, ocular involvement is often not present at birth and can occur decades after. For this reason, two to three inspections of the ocular fundus in the first year of life are recommended. Then annual inspections up to school age are advisable in order to recognize and treat an activation of the infection. Infection could pose a threat to the visual function at an early stage. Support should be offered to patients in their school and professional development in relation to their visual function when disorders occur or increase. In contrast, precautionary examinations do not appear to be helpful in the case of adult eye toxoplasmosis, as they do not allow prediction of the recurrence of the disease. Classically, the disease manifests itself through blurred or foggy vision as well as sense of mosquitoes in front of the eye. If these symptoms occur, an ophthalmological examination and a decision on the necessity of a therapy is of course necessary.
If patients with eye or brain toxoplasmosis simultaneously develop a serious general disease or a disorder of the immune system (due to medication following organ transplant or in the case of serious general diseases such as cancer or chemotherapy) the risk of activating the infection is particularly high. In such cases, a precautionary drug treatment with antibiotics to prevent the outbreak of toxoplasmosis is worth considering.
It is not clear what can trigger a resurgence of the disease. However, there are indications that stress, irregular day-night rhythms, excessive alcohol and drug consumption and all impairments of the immune system favor reasons for recurrences. Prevention or avoidance of the infection for life is theoretically conceivable. In practice though, it is hardly possible. Because of the normally minor problems in the case of a toxoplasmosis infection, outside of pregnancy, it is not advisable. In any case, prevention is advisable if a woman becomes pregnant without antibodies against toxoplasmosis. Women who have no antibodies against the pathogen should know the transmission route of the infection when they wish to have children or at the beginning of pregnancy and should try to avoid a fresh infection during pregnancy. To prevent a new infection with toxoplasmosis, not only is it important to avoid contact with raw meat or to wash one’s hands thoroughly afterwards, but also to wash one’s hands thoroughly after contact with soil and garden vegetables. Vegetables must be cleaned carefully before eating, as they may be contaminated with parasite cysts. All objects that may have come into contact with cats and cat excrement should be handled with special care during pregnancy. Cat owners, if pregnant, should take special precautions. Examples can be found on the website of the Robert Koch Institute of the Federal Health Office. If these precautions are followed, the risk of developing toxoplasmosis during pregnancy is low.
-
SUMMARY
In summary, toxoplasmosis is the most common infectious cause of uveitis. The pathogen, Toxoplasma gondii, occurs all over the world. It is assumed that 30 to 80% of all people become infected with it in the course of their lives. What leads to the manifestation of the eye (retinochoroiditis) is not known. A visual impairment is the result of foci at the point of sharpest vision (macula), which are more common in the congenital form. The eye diagnosis can be implemented clinically and chemically (via laboratory), if necessary. Diagnosis can be secured by a parallel examination of blood and ocular fluid in over 80%, but the congenital and acquired form cannot be distinguished by laboratory techniques. Toxoplasmosis breaks out again in about 60% at some point in the course of life (relapses). Triggers for these recurrences are not yet known, which means that recurrences cannot be prevented at present. The therapy aims to reduce the risk of permanent visual disturbances if a focal point threatens the center of the retina (macula). A prevention of eye toxoplasmosis recurrences is not known. Therefore, during pregnancy of women who have not been in contact with the pathogen before (= have no antibodies), primary attention must be paid to reducing the risk of infection.
-
RECOMMENDATIONS
Recommendations for the prevention of connatal toxoplasmosis
- What is toxoplasmosis?
Toxoplasmosis is an infectious disease caused by a microscopic parasite. About one third of the population is infected in the course of life, mostly without symptoms. Transmission occurs primarily through the consumption of raw or insufficiently cooked meat. - What does toxoplasmosis mean for pregnant women?
If a woman becomes infected during pregnancy, the infection can also be transmitted to the unborn child. In rare cases, this can lead to inflammation of the eyes and brain damage in the child. - How can I protect my child in the womb?
There are drugs that are effective against the parasite, but these are not able to prevent transmission to the child or symptoms in the child. Diagnosis or treatment of the infection during pregnancy is therefore not helpful. - Is there still a way to protect my child?
You can reduce the risk of toxoplasmosis for your child by taking a few simple precautions to reduce the likelihood of contracting the parasite during pregnancy. - What should I pay attention to in the kitchen and when eating?
Avoid eating raw (e.g. tartar rolls) or undercooked/roasted (bloody) meat (especially beef, lamb, poultry or game) during pregnancy. Wash your hands and kitchen utensils thoroughly if you have touched raw meat or offal. - Can I do more? In the house and garden? At work? If I keep a cat?
In cats, the parasite can multiply in the intestines and can therefore be excreted with the faeces and deposited in the environment. Even though the resulting risk of infection is considered to be rather low, it is still advisable to always wash your hands after touching sand or soil and processing fresh vegetables. Do not give your cat raw meat, but tinned food. The cat box should not be placed in the kitchen. Wear rubber gloves to clean the litter box and wash your hands afterwards. Good hand hygiene is also important if you work in a farm, restaurant, flower shop or pet shop.
- What is toxoplasmosis?